Wounds − Adapted from Dr. Duggan’s Geriatrics Guide¶
-
To do when admitting a patient with wounds:
- Document ALL wounds that are present on admission. This affects reimbursement
-
Use the Haiku app on your cell phone to document images of wounds in chart
-
Wound Service hours are Monday through Friday, 6 AM - 2 PM
-
If there is an urgent/emergent wound need (i.e. needs surgical eval or management), consult the appropriate surgical service
-
While awaiting consultation, initiate topical wound care orders (detailed below)
-
-
Consider contributing factors: nutritional, pressure-offloading equipment, wound supplies, PT/OT, home health nursing
Types of wounds¶
-
Arterial wound - Calciphylaxis
-
Venous leg wound - Fistula
-
Diabetic foot wound - Abscess
-
Vasculitis - Skin tear
-
Pyoderma gangrenosum - Pressure injury
-
Fungating lesion - Ischemic ulcers / gangrene
Vascular Wound Etiologies¶
-
Arterial: located on distal ends of digits, shallow, well-defined borders, pale/necrotic wound bed, minimal exudate due to poor blood flow, cramping pain or a constant deep ache
-
Diabetic: plantar surface of foot, callused wound margins; usually painless due to neuropathy
-
Venous: located on medial malleolus or gravity dependent areas, irregular edges, ruddy red with yellow slough and copious exudate
Pressure Injury Staging¶
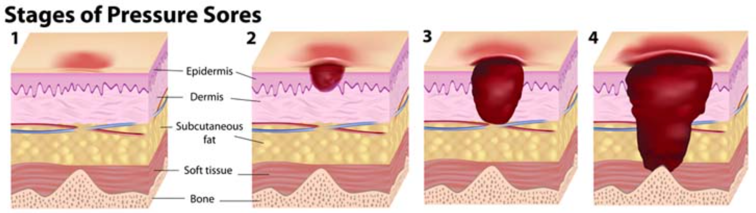
| Feature | Deep Tissue Injury | Stage 1 | Stage 2 | Stage 3 | Stage 4 |
|---|---|---|---|---|---|
| Skin Consistency | Boggy | Boggy | Variable | N/A | N/A |
| Skin color/nature of lesion | Non-blanching purple or maroon, may appear as blood-filled blister | Non-blanching erythema | Abrasion, blister, or shallow crater | Variable | Variable. If eschar, must be removed in order to stage, or is unstageable |
| Depth | Epidermis intact | Epidermis intact | Through surface of epidermis and outer dermis | SQ tissue to, but not through, fascia | Full-thickness loss w/ destruction, necrosis, or damage to muscle, bone, supporting structures |
Non-Acute Wound Consult Guidelines¶
-
Order “Inpatient Consult to Adult Wound" for these wound types: diabetic foot wounds*, venous, arterial, pressure injuries (consult required for DTI, stage 3, 4, and unstageable), IV infiltrate, skin tears, moisture-associated dermatitis, calciphylaxis, vasculitis, pyoderma gangrenosum, fungating lesion, abscess*, surgical wounds*, or wound VAC
-
*Diabetic foot wounds: if pt being followed by podiatry, order "Inpatient Consult to Podiatry"
-
*Abscess: if chronic due to IBD, consult colorectal surgery
-
*Surgical wounds: if pt has VUMC surgeon, consult the respective surgical service
-
Order "Inpatient Consult to Adult Ostomy / Fistula / Tube" for ostomy, trach, PEG, associated needs or complications (etc)
Acute Wound Consult Guidelines¶
- Abscess, hematoma, or osteomyelitis with overlying wound – whom to consult for drainage/debridement:
- Face – Face
- Chest/Sternum – CT surgery
- Breast – General surgery
- Spine – Spine
- Arm (hand to elbow) – Hand
- Lower leg (foot to knee) – Ortho
- Labial – OB/GYN
- Scrotal – Urology
- Buttock, thigh (knee to hip), arm (elbow to shoulder) – EGS consult
- Perirectal/Rectal acute abscess – EGS; (chronic due to IBD – Colorectal Surgery)
- Necrotizing Fasciitis – whom to consult for URGENT/EMERGENT surgical eval:
- Genitalia – Urology
- Buttocks, perineum, abdomen – EGS
- Upper extremity (shoulder to hand) – Hand
- Lower extremity (hip to toes) – Ortho
Wound Care (order while awaiting consultant recs)¶
- Superficial wounds
- Stage 1 or 2 pressure injuries, moisture-associated skin damage, or skin tears
- Order “Adult Skin Care Guidelines” and use the order set to guide you
- Stage 1 or 2 pressure injuries, moisture-associated skin damage, or skin tears
- Shallow Stage 3 pressure injuries (i.e., <1cm deep) or diabetic foot ulcers
- Order “Wound Care”: Frequency 2x weekly and prn; Cleanse with NS; protect periwound with Mepilex foam (type in comments)
-
Painful superficial wounds with no infection (i.e. vasculitis, PG, calciphylaxis)
- Order “Wound Care”: Frequency 2 times daily; Cleanse with NS; Apply Vaseline; Protect periwound with Xeroform and dry gauze (type in comments)
- If wound is on the hand, arm, foot, or lower leg consider wrapping in Kerlix
- If wound is on the trunk (i.e., abdomen or buttocks), consider covering with an ABD pad and secure with medipore tape
- Order “Wound Care”: Frequency 2 times daily; Cleanse with NS; Apply Vaseline; Protect periwound with Xeroform and dry gauze (type in comments)
-
Infected superficial wounds
- Odor alone does NOT indicate infection; wounds with necrotic tissue may have odor
- Order “Wound Care”: Frequency 2 times daily; Cleanse with NS, Apply Silvadene; Protect periwound with Xeroform and dry gauze (type in comments)
- If wound is on hand, arm, foot, or lower leg consider wrapping in a Kerlix
- If wound is on the trunk (i.e., abdomen or buttocks), consider covering with an ABD pad and secure with medipore tape
-
Medication order required: Silvadene q12h; in Admin Inst put “per wound care orders”
-
Deep wounds (i.e., stage 3, 4, or deep diabetic foot wound (all >1cm deep))
- Order “Wound Care”: Frequency 2 times daily; Cleanse with NS, pack with Dakin’s 0.025% (1/20 strength) soaked continuous Kerlix roll; Protect periwound with ABD pad & medipore tape (type in comments)
- If wound care is painful, consider changing to daily dressing changes
- Medication order required: Dakin’s 0.025% solution q12h; in Admin Inst put “per wound care orders”
-
Deep tissue injury
- Medication order required: Venelex (balsam peru-castor oil) ointment q4h; in admin instructions put location to apply ointment and put “no dressing”
-
Fungating mass
- Order “Wound Care”: Frequency 2 times daily; Cleanse with baby shampoo and water, NS, Metrogel (type in comments); Protect with Xeroform, ABD pad, medipore tape
- Medication order required: metrogel q12h; in Admin Inst put “per wound care orders”
-
Wound VAC
- Vanderbilt surgeon – consult Vanderbilt provider to provide care
- Ensure connected to VUMC wound VAC. Pt shouldn't use home unit while admitted
- Order “nursing communication” to “Obtain wound VAC hospital machine and canister from service center to connect pt to hospital machine.”
- Wound VAC should not be left without suction for more than 2 hours
- Settings: 125 mmHg continuous
- Vanderbilt surgeon – consult Vanderbilt provider to provide care
-
Non VUMC surgeon (i.e., gets wound care at outside hospital/wound care center)
- Discontinue wound VAC as soon as possible
- Remove all of the clear plastic drape just like you would remove tape
- Remove all of the sponge just like you would remove gauze packing
- Examine the wound to ensure no residual sponge by gently probing site
- Rinse with saline, initiate care based wound type as above
-
Leg wrap
- Ex: Unna's boot, ACE and 2, 3, or 4 layer compression
- Remove by cutting the wrap off
- Assess the wound and order dressing based on type of wound as above
- Order ACE bandage wrapped toe-to-knee. Remove q12h to assess skin