Basic Chest X-ray Interpretation¶
An X-ray is a density-gram where “white” is “dense” and “black” is “not dense.” Determine a systematic method you use every time you interpret a CXR to ensure you don’t miss anything
- Start every CXR you interpret by assessing the quality of the film:
- Penetration:
- Should see vertebral bodies through the cardiac silhouette but not into the abdomen
- If you cannot see them through the heart, the film is “under-penetrated,” and everything will appear more “white.”
- If you can see them through the abdomen the film is “over-penetrated” and everything will appear more “black.”
- Rotation: Spinous processes should be in the middle of the clavicular heads
- Two Different Systematic Methods:
-
ABCDE method
- Airway – Trachea midline and patent
- Bones – Bone density and obvious fractures
- Cardiac Silhouette – Should see L & R heart border, if not there
may be an adjacent opacity (Right Middle Lobe, Lingula)
- Cardiomegaly = heart size ≥ ½ the width of the hemithorax on a PA film
- Diaphragm – Look for pleural effusions at the costo-phrenic angle. If you cannot see the diaphragm along the way, there may be an adjacent opacity (Lower Lobe)
- “Everything else” – Refers to the lung fields
- Extra-Thoracic Soft Tissue – Subcutaneous emphysema
- Fields and Fissures –lung fields should appear symmetric and “black”
- Great Vessels – Tortuosity of the aorta and the outlines of the pulmonary vessels
- Hilum – Hilar masses, LAD and pulmonary arteries
-
Working around the film method:
- Imagine the entire CXR film as a square and an inner “box” as the pleural lining
- Outside the box: Lines/tubes, subq emphysema, gastric bubble, subdiaphragmatic air
- Edge of the box: Look for pleural thickening, pleural effusion, pneumothorax, visualization of the diaphragm
- Middle of the box: Trachea, vascular pedicle, hila, heart borders, great vessels, retrocardiac space
- The lung fields
Silhouette sign
- Two things of different densities will show a clear border on a chest x-ray
- Loss of a border you expect to see suggests a change in density of one of the structures.
- Ex: heart &l lung have different densities with sharp border. Loss
of this border suggests that the lung “increased” in density
- Ex: Pneumonia (fluffy opacities, air bronchograms, asymmetric) and pulmonary edema (linear opacities, fluid in fissures, Kerley B lines, cephalization)
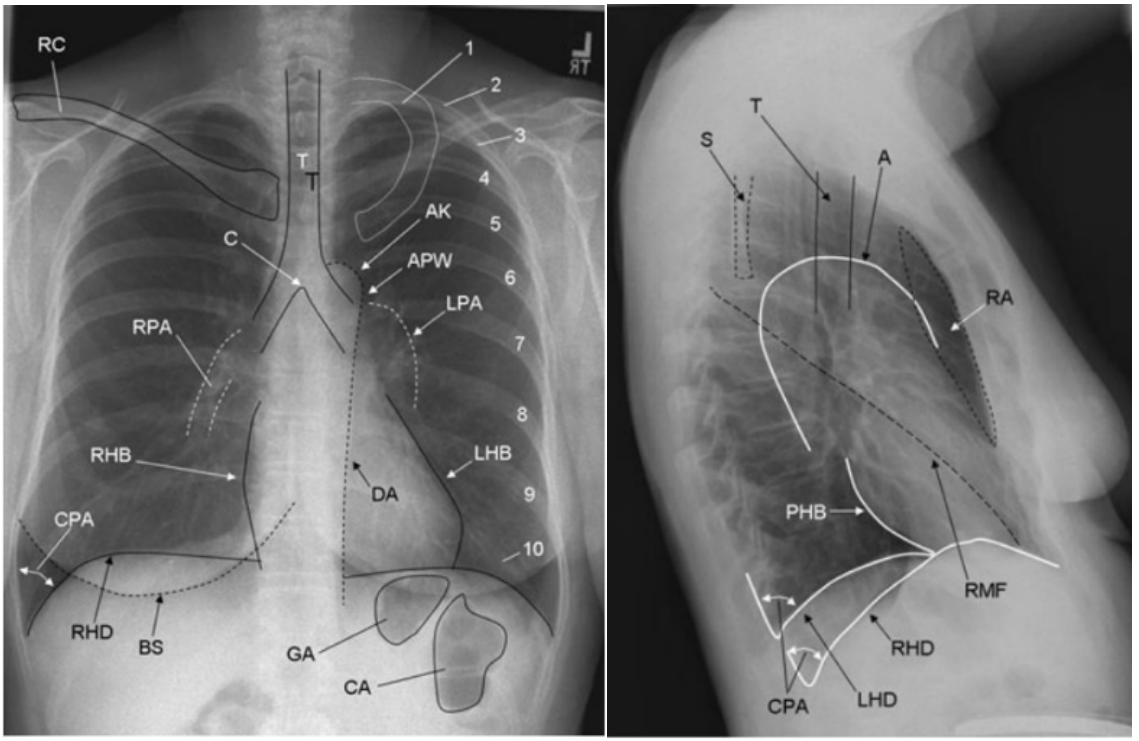
- 1,2-10: first rib, posterior aspect of ribs 2 to 10
- AK: aortic knob
- APW: aortopulmonary window
- BS: breast shadow
- C, T: carina, tracheal air column
- CA, GA: colonic air, gastric air
- CPA: costophrenic angle
- DA: descending aorta
- LHB: left heart border (most of which represents the left ventricle, the superior aspect represents the left atrial appendage)
- LPA: left pulmonary artery
- RC: right clavicle
- RHB: right heart border (represents the right atrium)
- PHB: posterior heart border
- RHD, LHD: right hemidiaphragm, left hemidiaphragm
- RPA: right pulmonary artery
- S: scapula
- RA: retrosternal space
- RMF: right lung fissure (left major and minor fissures are not always visualized)
Chapter 15. Imaging Studies. Gomella L.G., & Haist S.A. (Eds.), (2007). Clinician's Pocket Reference: The Scut Monkey, 11e. McGraw Hill. https://accessmedicine.mhmedical.com/content.aspx?bookid=365§ionid=43074924